How to treat gluteal tendinopathy – What actually works?
- Maryke Louw

- May 13
- 17 min read
Updated: Jun 24
Recovering from gluteal tendinopathy can feel frustratingly slow, especially when everyday activities like walking, sitting, or sleeping keep aggravating the pain. The good news is that most cases improve with the right combination of rest, exercise, and avoiding specific movements – like stretches – that irritate the injured tendon.
In this guide, we explain which treatments for gluteal tendinopathy are backed by research, which ones might help in certain situations, which approaches are best avoided, and how long you might take to recover.
Remember, if you need help with an injury, you're welcome to consult one of our physios online via video call.

The terms tendinitis, tendonitis, tendinosis, and tendinopathy mean the same thing for all practical purposes, and we use these interchangeably in our articles. Read more (opens in new window).
In this article:
We've also made a video about this:
The main elements of effective treatment
We can summarise what happens when you get gluteal tendinopathy as follows:
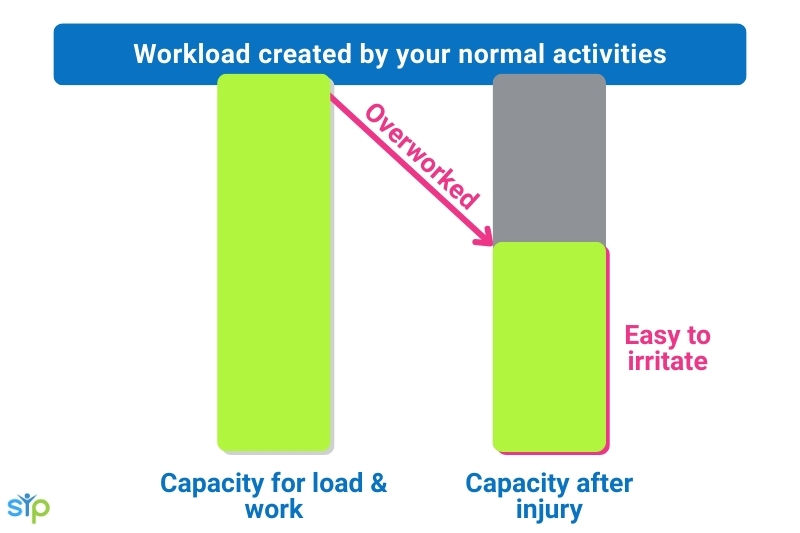
Your glute tendons get injured when they are overworked in some way (see the most common ways here).
Once injured, your tendons (it is often more than one that is affected) become irritated and their capacity to tolerate load or work reduces.
This means that when you now try to do the things you usually do, it’s too much for the tendons and they become even more irritated.
Women are especially prone to developing this injury during any stage of the menopause due to the drop in estrogen which slows your tendons’ ability to recover after physical activity.
There is no one-size-fits-all treatment plan that works for gluteal tendinopathy, but the main aims of a successful treatment plan are to:
get the tendons to calm down and reduce their irritability
restore the tendon’s load tolerance and capacity to its previous level (and beyond)
take steps to prevent the tendons from being overwhelmed and injured in future.
💡 In practice, these three aims can be achieved through many combinations of various treatments, and what works for one person often doesn’t work that well for the next.
So, let’s look at the elements you might include in a treatment plan, starting with the best research-based ones.
What treatment works best for gluteal tendinopathy?
These are our Top 3 treatments – supported by the research and that we find produce the best long-term recovery when used together:
Relative rest: For your injury and pain to settle and start recovering, you must temporarily reduce the loads or forces that go through that area to match its current capacity. But usually you don’t have to rest it completely – more on this below.
Progressive loading: As your pain starts to calm down and settle, you must gradually start increasing activities that load/work the gluteal tendons. This helps to restore the strength and function of the injured tendon and related muscles, and it reduces pain. This includes your daily activities as well as your rehab exercises (see below) and sport.
Addressing other factors that might be dialling up the pain system and causing more pain than they should.
We discuss each of these treatments aspects in detail below.
💡 If you have an inflammatory condition (autoimmune, gout, etc.), speaking to your doctor about your medication should be the first step. The other treatments discussed in this article will only work if your inflammatory condition is under control.
1. Relative rest vs. complete rest
Resting your glute tendons completely (not doing any exercise) can be a very effective way to get the pain to settle down in the short term. And this is sometimes needed for a short period (a few days only).
But rest alone doesn’t restore your tendons’ capacity for exercise and work. And if you rest for very long periods, your tendons may decondition further (just like your muscles would without exercise). Research has also shown that overprotecting an injury can sensitise the pain system and cause more pain in the long term.
⚖️ So, like with most things in injury rehab, it’s about getting the balance right.

👉 What you want to do instead is reduce, adapt, or cut out only the activities that significantly aggravate your glute pain and continue with the others that don’t.
Then, once your pain has settled down to an acceptable level (as discussed below), you gradually start easing back into those activities, testing short sessions or durations and observing how it affects your symptoms.
👍 We are big proponents of relative rest and teach all our online patients how to apply this concept to their specific case. Being injured and not able to exercise can make you feel rather low. Relative rest is great, as it not only allows you to maintain your fitness through cross-training but also helps to lift your mood.
How much pain is OK?
We’re often asked “Should I wait until I have no pain before starting physio?” The answer is, no, you are unlikely to get 100% pain-free if you just rest and don’t start rehab.
But with rehab I don’t mean exercises that are hard to do or cause your pain to flare up – an experienced physiotherapist will tailor your rehab plan so that it matches your tendons’ capacity, using a variation of the pain guide below.
✅ When you’re dealing with any type of tendinopathy (including gluteal tendinopathy), the general rule is that you can keep doing an activity as long as:
the activity only causes a slight increase in discomfort while you’re doing it or within the next 24 hours, and
that extra discomfort settles down fairly quickly.
⬇️ If your symptoms flare up more noticeably – especially the day after – that’s your cue to take the next session easier.
A significant increase in pain doesn’t necessarily mean that you’re making your injury worse, but repetitively pushing into high levels of pain can cause the pain system to become more sensitised, which can cause pain to persist long after the tendon tissue has recovered. Read more about the factors that can contribute to ongoing pain here.
👍 Tailoring your activities (exercise, walking, sitting, rehab, work, etc.) to keep your symptoms within this “niggle” level (1 to 2 out of 10) helps to calm the pain system down.
Activities that often require adapting during the early stages include:
Activities or positions that press directly on the injured tendons, e.g. sleeping positions. This doesn’t cause the injury to get worse, but often increases your pain in a similar way to how prodding a bruise makes it hurt more – find advice about sleeping positions for gluteal tendinopathy here.
Activities that use or work the glute tendons, e.g. standing, walking, running, cycling, squats, deadlifts, etc.
Movements that stretch the glute tendons, e.g. crossing your legs when you sit, bending forward or lifting your knees up to your chest, or doing glute stretch exercises. Stretching the tendons causes them to pull tight over and press against the bone on your outer hip (femur) which often irritates the tendon (“pressing the bruise” again).

You can find much more detailed advice on adapting specific activities for gluteal tendinopathy in these articles of ours:
How to adjust your sleeping positions to not push or pull on the tendons
Tips on how to sit with gluteal tendinopathy so it doesn’t irritate the tendons.
2. Progressive loading
Relative rest is great for allowing your injury symptoms to settle, but to fully recover, you have to gradually restore your injured tendons’ strength and tolerance for work over time.
Tendons are made up of collagen fibres, which is an extremely tough type of tissue – researchers report it to be 10 times stronger than steel! And you can get the body to produce more and stronger collagen fibres through training your tendons, just like muscle cells strengthen and grow bigger when you train them.
The aim with progressive loading is to restore your tendons’ strength and capacity to tolerate activities (like walking, standing and exercise) to their pre-injury levels.

If you do this correctly, using your symptoms to guide your loading plan, it can also be a great way of desensitising the pain system and getting it to calm down.
There are two ways of restoring your tendons’ capacity, and most treatment plans use a combination:
Specific rehab exercises that strengthen the gluteal muscles and tendons.
Gradually increasing the time you spend on your feet e.g. standing, walking, and running.
👎 Some of the common mistakes (regardless of the activity) we see which can cause painful flare-ups include starting specific activities too early, doing too much too soon, or not progressing exercises to the level required for your sport.
👍 Here are the steps we follow during our video consultations with our patients to help us figure out where to start a rehab plan, how and when to progress it, and what level to build it up to:
First, we have a very detailed discussion with our patients to understand what activities they are currently able to do and how it affects their symptoms – this gives us an idea of what activities they might need to adapt or adjust or do more of.
We also discuss what our patients’ goals are – that tells us what type, volume, and intensity of activity their plan should build up to.
We are also interested in unpacking the details about how the symptoms started – that tells us what other factors might have contributed to their injury and what our patients should do to avoid getting gluteal tendinopathy again.
Then we move on to movement tests to understand what exercises might be appropriate. We use the same movements we would use in a physical clinic – we demonstrate the movements in front of the camera, then watch the patient do them, and give feedback.
We then use this information to create a starter plan – but this often has to be adjusted after the patient has had time to test it and observe its effect.
Our patients then provide us with feedback in the subsequent consultations and we use that to decide how to proceed – if they should continue at the same level, can progress, or perhaps should take things a bit easier.
Getting your loading plan right is not an exact science and often takes a bit of experimenting because you have to look at ALL the activities in your day/week that impact the gluteal tendons and match that to what your tendons can currently tolerate.
Tendons can also be tricky things, and they sometimes only tell you hours after an activity or even the next day that they didn’t like it. If you find your rehab exercises are irritating your tendons, don’t just give up on it, tell your physio so they can use this new information to further fine tune your plan.
You can find more detailed information about specific gluteal tendon rehab exercises that might be useful or are best to avoid in this article.




3. Address other factors affecting pain
Recent research has highlighted how tendon pain can be amplified or reduced by increasing or decreasing our stress and anxiety levels.
We’ve explained it in detail here, but in a nutshell, stress and anxiety cause our bodies to produce more stress hormones (like cortisol) which, if produced over a prolonged period, can cause increased inflammation and tissue hypersensitivity.
This might cause our pain system to overreact to movement and activity and cause excessive pain flare-ups even when the activity is not vigorous enough to injure our tendons.
If you’re currently experiencing high levels of stress or anxiety, taking steps to address this might help your recovery.

Other treatments that might promote tendon healing
The treatments below are thought to promote tendon healing, and there is some research evidence that they can improve recovery when combined with other treatments.
PRP injections are thought to stimulate tendon healing, and there is evidence that they can help with gluteal tendinopathy recovery. In practice we find that it works for some people and not for others, so it’s not something we advise people to have routinely. However, if they are unable to make progress despite doing the right things as described above, this is a treatment worth considering.
Red light therapy – evidence is emerging that it likely stimulates healing and reduces pain. For tendinopathies, it’s been found to reduce pain and improve function – researchers report even better improvements in function when combined with rehab exercises. Here’s our comprehensive guide on how to use red light therapy.
Supplements – There is some evidence that a combination of Vitamin C and collagen, when combined with strength training exercises, may enhance your tendon’s ability to restore and strengthen itself. Find a detailed discussion of supplements for tendon injuries here.
Nitroglycerin patches – There’s currently a lack of high quality research for this, and studies show contradictory results, but these patches don’t seem to have any serious side effects. So it might be something worth trying if you find you’re not progressing as expected with your rehab. (Nitroglycerin, trinitroglycerin (TNG), nitro, glyceryl trinitrate (GTN), and 1,2,3-trinitroxypropane are different names for the same thing.)
PDRN injections (popularly known as "salmon sperm injections") are also thought to stimulate tendon healing and help with pain relief, with initial research showing promising results and no serious side effects. But because the studies into this have been small thus far, it should be seen as experimental, and it might or might not work for you.
Treatments to reduce pain
You might wonder why it’s worth bothering with treatments that only target the pain symptoms, but getting your glute pain to settle down to a manageable level is important.
Pain can wear you down, prevent you from getting on with your life, and discourage you from starting or progressing with your rehab exercises. And if it affects your sleep, it can have all sorts of knock-on effects.
The following treatments can help to reduce your pain temporarily, but they usually don’t have a direct effect on healing and should not be used as a stand-alone solution. For best results, they should be used in combination with the three core treatment components we discussed above.
Going for a massage or doing self-massage using a massage ball or massage gun can be useful as long as you avoid strong pressure over the irritated gluteal tendons – rather focus on the muscles. In our experience, very gentle massage tend to work much better than deep tissue or trigger point therapy, which often leads to flare-ups.
Taping the gluteal and lateral hip area. This hasn’t been researched much. The only study currently published reported equal improvements in pain with both the proper and sham taping techniques compared to participants with no tape, which makes me think it was down to placebo rather than any true treatment effect. But tape is relatively cheap and easy to apply yourself, which makes it a low-cost experiment – we find it works for some patients and not for others.
Dry needling. A 2022 review study found that it effectively reduced pain and other symptoms linked to tendinopathy. These results are echoed by another review that found it to be as effective as a corticosteroid injection in reducing gluteal tendinopathy pain.

Dry needling can help to reduce gluteal tendinopathy pain – but only if you're not afraid of needles. Low-level laser therapy has been proved effective for reducing pain, without any negative side effects.
Shockwave might help to reduce pain, but it doesn’t work for everyone. The research-based recommendation is that shockwave should only be used for tendinopathies that have lasted longer than three months and aren’t improving as expected.
Ice can work well for pain relief, but shouldn’t be overused – find a detailed guide here.
Heat is also an option, as long as your injury is more than three months old – it’s generally not advised to use heat when there’s inflammation, which might be the case during the early days or when you experience flare-ups.

TENS (transcutaneous electrical nerve stimulation) has been shown to effectively reduce pain while the machine is on you, and the effect might last for a few hours after.
Losing weight. Research shows that carrying extra fat – particularly around the waist – can alter blood chemistry, trigger chronic inflammation, and make tendons less healthy and slower to heal.
High-volume injections consisting of normal saline (clean water) plus anaestetic and a small amount of corticosteroid appear safe and effective for pain relief in tendons.
Treatments for specific cases of gluteal tendinopathy
These treatments are not generally advised, because they might have unwanted side effects or are only effective under certain circumstances. However, when used at the correct time, they can be beneficial.
Arch support insoles or orthotics. If you overpronate (foot rolls in excessively) as you walk or run, it might cause your leg to follow and turn in excessively, which in turn can increase the force on the gluteal tendons. Arch support orthotics can help to reduce excessive pronation, which in theory should help with recovery in these cases.
So far no research study has specifically looked at how effective these insoles are for people who overpronate and have gluteal tendinopathy – the two available studies included patients who don’t overpronate, which likely explains why they showed contradictory results.

Hormone replacement therapy (HRT) might improve healing if you’re in the menopause. Oestrogen is one of the main hormones in charge of getting your tendons to produce new and stronger collagen fibres (the main building block of a tendon). The drop in oestrogen levels due to the menopause has been shown to both be a risk factor for developing tendonitis and to slow healing.
Anti-inflammatory medication might be useful if you have hip bursitis, inflammatory enthesopathy, or if your tendonitis was caused by antibiotics or an inflammatory condition like gout or arthritis. It is usually not effective for ongoing gluteal tendinopathy caused by overload.
Corticosteroid injections are a bit controversial – in a recent review of the available research that looked at steroid injections vs. placebo for gluteal tendinopathy, researchers found that it might reduce pain in the short term but does not seem to have any positive long-term effect.
There is also research that suggests that it might not be great for long-term recovery and should therefore be used sparingly. That said, some cases of gluteal tendinopathy can be super stubborn and just don’t want to react to any other treatment. If that is the case, corticosteroid injections might be an option to try before considering surgery.
Surgery (bursectomy or tendon repairs) might be an option in cases of gluteal tendinopathy where no other treatments bring relief. It does bring relief for some patients, but due to a lack of research, there are currently no clear guidelines on when a patient is most likely to benefit from it. The current advice for tendinopathy in general is to consider surgery only if you’ve tried a progressive rehab plan (as described above) for at least 12 months.
Tenex (a type of minimally invasive surgery) might help to reduce pain and improve function by removing the injured part of the tendon and is less invasive than open surgery, but the current research that specifically looked at Tenex for gluteal tendinopathy suggests that, while it might reduce pain, it is no more effective than PRP injections.

Useless treatments for gluteal tendinopathy
These treatments are either a waste of time and money and/or might be bad for healing.
Therapeutic ultrasound. This is a very popular treatment used in clinics and is generally safe to use, but its effectiveness is questionable. Animal studies show it has the potential to positively affect tendon healing, but when tested on real patients and compared to other treatments, it usually fails to show any benefit.
Corticosteroid tablets. These should never be prescribed as a treatment for tendon injuries. They are different from injections in that they have a systemic and more long-term effect, and there is much stronger evidence for the detrimental effects tablets might have on tendon health.
💡 BPC-157 peptides. Although there’s a lack of research into their safety and effectiveness in humans, these peptides are widely promoted online as being helpful for healing. We don’t recommend them, as they are experimental and their long-term safety is unknown.
Treatments that might make your symptoms worse
These treatments irritate or worsen symptoms in most people with gluteal tendinopathy. However, we are all different, and some people will find these treatments don’t affect them or perhaps even beneficial.
Glute stretches. As mentioned earlier, these types of movement cause the gluteal tendons to compress strongly against the outer hip bone, which usually increases pain.

Very strong massage. Even when the pressure is on the gluteal muscles and not directly on the tendons, very strong pressure seems to flare up most cases of gluteal tendinopathy.
Prolonged periods of rest. Resting your tendon for short periods when needed is important. But long periods of rest with very little activity can actually make it feel more uncomfortable (due to reduced circulation) and cause your tendon to lose even more strength. Applying the concept of relative rest is much more effective in the long run.
Recovery times
💡 You can sometimes see quite dramatic improvements in pain as soon as you stop doing obvious things that have been irritating your tendons (like stretching the glutes).
But in cases where there are no obvious triggers to cut out, it usually takes between 4 and 12 weeks to really start noticing significant improvements in your function – it takes time for rehab exercises to strengthen the tendons.
Full recovery tends to take at least 6 months, but often more (12 to 18 months).
Every case is different, and recovery time is influenced by several factors, including:
How long you've had your symptoms – the longer you have pain, the more sensitised the pain system becomes and the longer it takes to get it to calm down again.
Your tendons’ stage of injury – tendon injuries in Stage 1 (reactive tendinopathy) recover more quickly than ones in Stage 3.
How effectively you can implement the correct balance between rest and loading – sometimes one's work or daily tasks mean that you have to continue with things that irritate the tendon, which can make recovery take a bit longer.
How well you’re addressing the “extra” factors that can impact pain, e.g. stress and anxiety – these factors can sometimes cause pain to persist long after the tendon has already regained its capacity.
How we can help
Need help with an injury? You’re welcome to consult one of the team at SIP online via video call for an assessment of your injury and a tailored treatment plan.

We're all UK Chartered Physiotherapists with Master’s Degrees related to Sports & Exercise Medicine or at least 10 years' experience in the field. But at Sports Injury Physio we don't just value qualifications; all of us also have a wealth of experience working with athletes across a broad variety of sports, ranging from recreationally active people to professional athletes. You can meet the team here.







About the author
Maryke Louw is a chartered physiotherapist with more than 20 years' experience and a Master’s Degree in Sports Injury Management. Follow her on LinkedIn and ResearchGate.